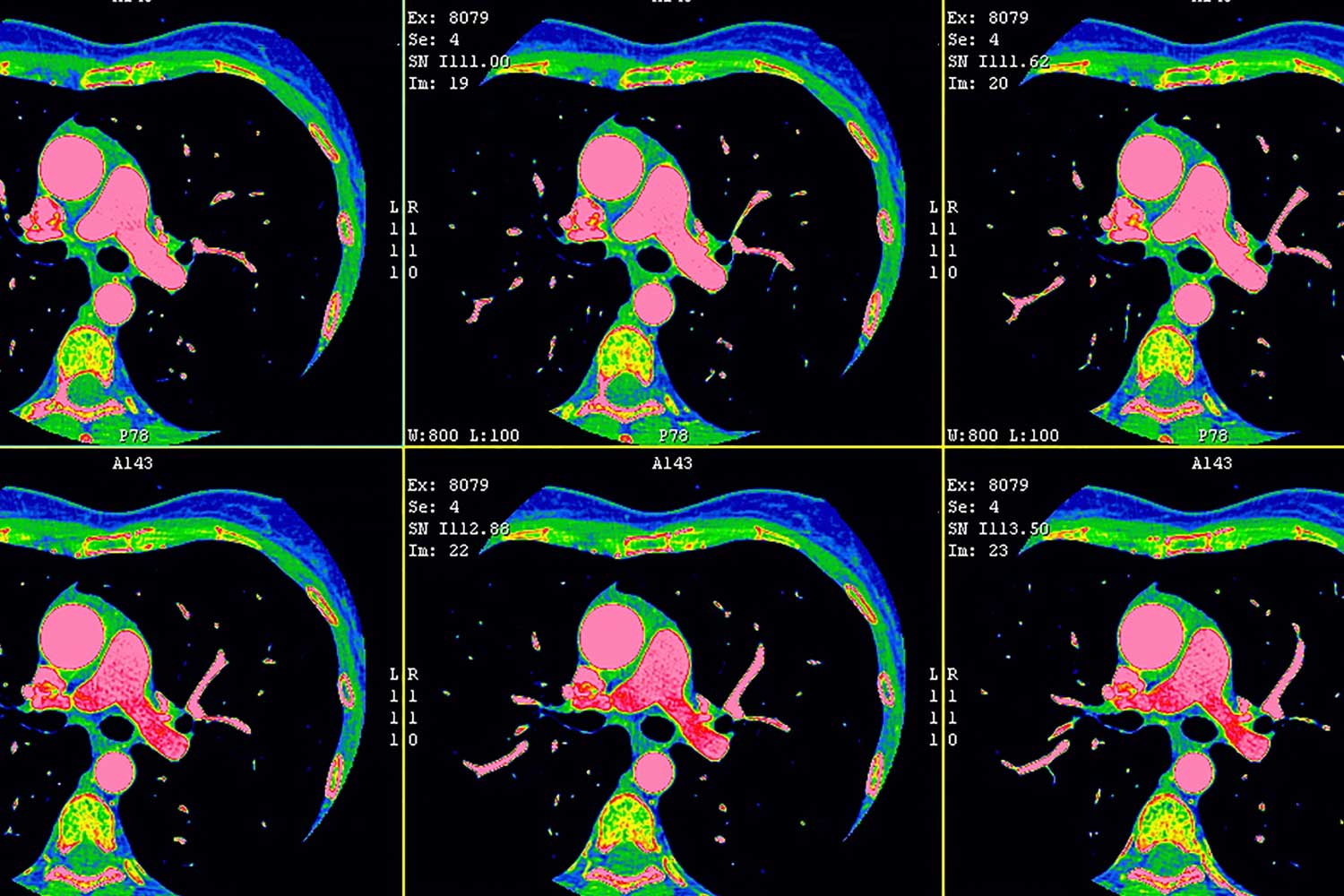
Quantitative plaque analysis using cardiac CT angiography (CCTA) provides an accurate assessment of arterial plaque and could dramatically impact the management of patients with diabetes who face a high risk of heart attacks and other cardiovascular events, according to new research.
Quantitative plaque analysis using cardiac CT angiography (CCTA) provides an accurate assessment of arterial plaque and could dramatically impact the management of patients with diabetes who face a high risk of heart attacks and other cardiovascular events, according to new research.
Plaque that forms in the arterial walls can restrict blood flow and, in some cases, rupture, leading to potentially fatal heart attacks. There is considerable evidence that calcified (stable) plaque is less prone to rupture than noncalcified (soft) plaque. Intravascular ultrasound can quantify noncalcified and calcified coronary artery plaque but is an invasive procedure unsuitable for screening purposes. Coronary artery calcium scoring with CT also has limitations.
“Calcium scoring measures how much calcified plaque a person has, but it doesn’t measure the component that’s not calcified, and that’s the component that tends to be dangerous,” says João A. C. Lima, MD, of the cardiology division at Johns Hopkins University in Baltimore.
Quantitative plaque analysis with CCTA has emerged as a viable screening option. It can capture the full anatomic map of the coronary arteries in a single heartbeat with low radiation dose and can provide a picture of the total amount of plaque throughout the arteries of the heart.
Researchers from the National Institutes of Health (NIH), Johns Hopkins, and the Intermountain Medical Center Heart Institute in Salt Lake City collaborated to evaluate CCTA in 224 asymptomatic patients with diabetes. Obese people with diabetes have a propensity for extensive and premature development of coronary artery plaque, making them an ideal study group for plaque assessment.
The researchers used measurements of coronary artery wall volume and length to determine a coronary plaque volume index for each patient. The technique provided information well beyond the presence or absence of coronary stenosis. Plaque volume index was related to age, male sex, BMI, and duration of diabetes. Younger individuals with a shorter duration of diabetes had a greater percentage of soft plaque.
“Coronary plaque volume index by CCTA is not only clinically feasible and reproducible in patients with diabetes, it provides a more complete picture of the coronary arteries that could be routinely applied in at-risk patients,” says David A. Bluemke, MD, PhD, of the NIH Clinical Center.
In the study, BMI was the primary modifiable risk factor associated with total and soft coronary plaque as assessed by CCTA. “The results reinforce how important it is to evaluate BMI as a potential driver of overall diabetes,” Bluemke says. “As the only modifiable risk factor, obesity is an important target for managing diabetic patients.”
Only about one-third of the coronary plaque in study patients showed calcification, underscoring the widespread presence of noncalcified plaque. The ability to distinguish between calcified and noncalcified plaque is important because treatment may vary based on plaque composition. “People with soft plaque respond better to interventions, particularly medical therapy like statins,” Lima says.
The researchers will continue monitoring the study patients to better understand the value of coronary artery plaque assessment in predicting future cardiovascular events and to further define the role of plaque volume index vs. coronary artery calcium score. A clinical trial would be necessary to determine whether risk factor reduction would result in reduced plaque volume index.
“Now that we have baseline indices of plaque in the study patients, we can look for people who, despite optimal management, experience a cardiovascular disease event like a heart attack,” Bluemke says.
The researchers also noted that CCTA and quantitative plaque analysis may prove valuable for other groups of patients at high risk of cardiovascular events and may one day enable physicians to predict plaque development and treat it aggressively before plaque volume index increases significantly.
Source: Radiology Today